CASHRA Annual Conference 2012
June 18, 2012
Winnipeg, Manitoba
Ivan Zinger, J.D., Ph.D.
Executive Director and General Counsel
Office of the Correctional Investigator of Canada
Canadian Corrections by the Numbers
The Office of the Correctional Investigator: Role and Mandate
OCI by the Numbers
Top '10' Areas of Complaint to the OCI
A Human Rights Lens in Corrections
Legal Obligations
Definition of Mental Health
DSM-IV
Mental Health in Corrections
Prevalence of Mental Health Issues
Mental Health and Federal Corrections
Chronic Self-Injury in Federal Corrections
Concluding Remarks
Canadian Corrections by the Numbers
Federal Adult Corrections (2011-12)
- Offenders serving sentences of two years or more.
- 13,800 male and 600 women inmates.
- 8,600 offenders under community supervision.
- 18,500 people employed by the Correctional Service of Canada ( CSC ).
- CSC manages 57 federal penitentiaries (including 5 regional women's facilities), 5 regional treatment centres, 6 community correctional centres, and 92 parole offices.
- $3.0 B budget in FY 2011-2012 (a 40% increase from FY 2005-06), but $295M cut via Deficit Reduction Action Plan.
- Average annual cost of maintaining a federal inmate:
- $111,000 per male inmate; and
- $211,000 per woman (FY 2009/10).
- CSC adding 2,700 new cells in the next 2 years.
- CSC closing 3 institutions (1000 inmates) in the next 3 years
Provincial Adult Corrections (2009/2010)
- Offenders serving sentences of less than two years.
- 23,700 incarcerated provincial inmates (including 13,600 remand).
- 109,400 provincial offenders on probation and parole.
- Great majority of provinces are building new cell capacity.
Incarceration Rate by Province

2010 rate per 100,000 adult population: 141*
*Numbers include federal, provincial and territorial incarceration rate
(Source: Statistics Canada)
The Office of the Correctional Investigator: Role and Mandate
- The Office of the Correctional Investigator ( OCI ) acts as an Ombudsman for offenders under federal jurisdiction (serving a sentence of two years or more).
- The Office was formally entrenched in legislation in November 1992 with the enactment of the Corrections and Conditional Release Act ( CCRA ).
- The Act gives the OCI broad authority and the responsibility to investigate offender complaints related to "decisions, recommendations, acts or omissions" of CSC .
OCI by the Numbers
2010-2011
- Investigators cumulatively spent 376 days in federal penitentiaries.
- Interviewed over 2,100 offenders.
- Responded to close to 6,000 offender complaints.
- Conducted over 1,000 use of force reviews and reviewed 131 cases of serious bodily injury or death.
- Recorded over 20,000 toll free contacts.
Top '10' Areas of Complaint to the OCI
CATEGORY | # | % |
|---|---|---|
Health Care | 741 | 12.53% |
Conditions of Confinement | 469 | 7.93% |
Cell Effects | 407 | 6.88% |
Transfer | 369 | 6.24% |
Staff | 347 | 5.87% |
Administrative Segregation | 346 | 5.85% |
Grievance | 284 | 4.80% |
Information | 202 | 3.42% |
Programme / Services | 188 | 3.18% |
Telephone | 168 | 2.84% |
A Human Rights Lens in Corrections
- The business of Corrections is all about promoting respect for human rights; preventing human rights abuse; and, detecting and remedying human rights violations.
- When government has exceptional authority over its citizens, the potential for abuse of powers is great and the protection of fundamental rights must be a core preoccupation of those empowered and trusted with those exceptional powers.
- Every aspect of a prisoner's life is heavily regulated. The CSC makes thousands of decisions every day which impact on prisoners' fundamental rights.
"Federal penitentiaries are fast becoming the nation's largest psychiatric facilities and repositories for the mentally ill" Howard Sapers, Correctional Investigator, 2010
Legal Obligations
- The CCRA provides that the Correctional Service "shall provide every inmate with essential health care and reasonable access to non-essential mental health care that will contribute to the inmate's rehabilitation and successful reintegration into the community."
- The Service is further obligated to consider an offender's state of health and health care needs in all decisions, including placement, transfer, segregation, discipline and community release and supervision.
Definition of Mental Health
According to the World Health Organization ( WHO ):
- "Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. Mental Health is a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community. In this positive sense, mental health is the foundation for individual well-being and the effective functioning of a community."
According to the WHO definition, MH is described as more than the absence of mental disorders or disabilities.
DSM-IV
- The Diagnostic and Statistical Manual of Mental Disorders (4th edition) is the resource used in North America to define mental disorders.
- The manual is divided into five areas or axes:
- Axis I - Clinical Disorders
- Axis II - Personality Disorders and Mental Retardation
- Axis III - General Medical Conditions
- Axis IV - Psychosocial and Environmental Difficulties
- Axis V - Global Assessment of Functioning
- NOTE: Axis I = Major Mental Disorders
Mental Health in Corrections
Percentage of Prison Population with Mental Health Concerns
Narrow Definition of
Mental Health Illness
- Require Psychiatric Hospitalization for Acute Axis I Disorders (6-8%)
- Serious mental illness - psychotic, Bipolar, and major depressive disorders (14%)
Broader Definition of
Mental Health Illness
- Require Psychiatric Involvement (15- 20%)
- Require Psychological or Psychiatric Services (36%)
- Personality Disorders (75% Anti-social Personality Disorder)
- Previous history of substance abuse (80%)
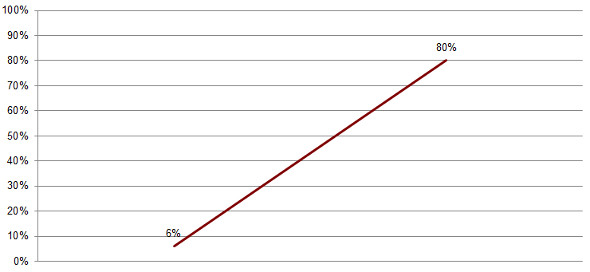
Prevalence of Mental Health Issues
Prevalence data in federal corrections are at best estimates: methodological and definitional issues
- Broad or narrow variables to operationally define MH illness:
- Psychiatric hospitalization for acute SMI (6-8%).
- Axis 1 diagnoses, prior psychiatric hospitalization, or on psychotropic medication (doubling between 1997 to 2008 - from 7% to 13%).
- Serious Mental Illness ( SMI ): psychotic, bipolar and major depressive disorders (14%).
- Personality Disorders: Anti-Social Personality Disorder (75%).
- Current vs. lifetime prevalence:
- Snapshot data vs. history of current and prior diagnoses.
- Need for psychiatric or psychological services:
- Identified at intake as requiring some level of psychological or psychiatric services (ComHISS, 36%).
Mental Health and Federal Corrections
Offenders with MH issues are more often:
- Victims of violence, intimidation and bullying.
- Placed in administrative segregation.
- Classified at higher security levels.
- Unable to complete correctional programs.
- Released later in their sentences.
Summary of OCI findings:
- Over last decade, significant increase of offenders being admitted into federal custody with MH issues.
- Needs for psychological and psychiatric services exceed capacity of CSC to provide adequate MH services.
- A few offenders with serious acute MH disorders and who chronically self harm should not be in Correctional facilities.
Reality for Some Offenders with MH Issues
Segregation 
Pinel Restraint 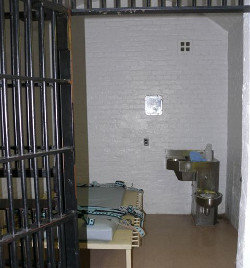
Chronic Self-Injury in Federal Corrections

- In FY 2011-2012, there were 1055 incidents of self-injury within the total inmate population (882 incidents in FY 2010-11):
- Among women offenders, there were 253 incidents of self-injury, including:
- 236 self-inflicted injuries (5 women accounted for 69% of these incidents).
- 14 attempted suicides.
- Among male offenders, there were 802 incidents of self-injury, including:
- 678 self-inflicted injuries (10 men accounted for 23% of these incidents).
- 37 attempted suicides.
- Among women offenders, there were 253 incidents of self-injury, including:
- Chronic self-injury offenders frequently results in:
- Prolonged periods in administrative segregation.
- Prolonged periods and repeated use of physical restraints.
- Use of force interventions.
- Multiple transfers to and from the regional psychiatric centre, complex needs unit or outside psychiatric facilities.
- Inter and intra-regional institutional transfers to provide staff respite.
- Offenders who self-injure may view traditional correctional interventions as punitive:
- Suicide watch.
- Segregation placements.
- Use of restraints.
- Video surveillance.
- Women offenders self-report that they engage in self-injury as a coping mechanism to deal with negative emotions, or to communicate with others about their problems and their need for care.
- The most common emotions reported by women prior to engaging in self-harm are: anger, depression, anxiety and being upset.
- Male offenders self-report that they engage in self-injury for instrumental reasons - to make a statement, to reinforce demands on staff, to protest a disciplinary measure.
- The most common emotions reported by men prior to engaging in self-harm are: anger or frustration, depression, anxiety and stress.
- Need to explore the relationships between conditions of confinement (i.e. isolation, seclusion, deprivation) and propensity for self-injury.
- Use of force interventions by correctional staff that are intended to cease or manage self-injury (i.e. restraints) may be counter-productive in reducing severity or frequency of self harm.
- The consistent use of MH care professionals as first responders, de-escalation techniques, individual treatment, and assessment-based clinical management plans yield better results.
- Long-term segregation and a more restrictive regime can increase the motivation for, severity and frequency of self-injury.
Concluding Remarks
- Upstream investments in community MH services, inclusive of prevention, diversion (e.g., MH and drug courts), anti-stigma campaigns, and enhanced multi-sectoral services related to mental health issues (e.g., housing, education, assisted living).
- To monitor progress, the development of performance indicators, sound prevalence data and an evaluation framework, which rely on common definition of MH .
- Investments in appropriate MH services in Corrections, including the creation of intermediate care units in federal correctional facilities.
- Implementation of alternative models of delivery of mental health services for some offenders. Acute psychiatric cases and persons who chronically self-harm should not be in a correctional setting.
- Offenders with serious MH issues should not be subject to long term segregation.
- Endorsement of a patient advocate model in federal Corrections.
Last Thought
"Addressing the high prevalence of mental health concerns in Corrections is not only a public health issue, but a human rights issue".
Date modified
2013-09-16
